
Minimally Invasive
Achilles Rupture Surgery
Written by Dr Mike Smith
You have ruptured your achilles tendon and want to know your best option
This guides outlines the new minimally invasive techniques available for surgical repair of a ruptured achilles tendon
An achilles rupture can occur spontaneously. It can also be seen in people that have had a vague pain or ‘tightness’ at the back of their calf for a period of time. In this scenario, the tendon has usually undergone a degree of degeneration prior to the ‘acute’ injury.
An achilles rupture is most frequently seen in middle aged recreational sporting enthusiasts, although it can occur in many age groups.

Achilles Rupture
There are 3 possible sites of achilles tendon ruptures:
Watershed Zone
This is the most common site of tendon rupture and is located 3-5 cm above the achilles tendon insertion into the heel bone (calcaneus). The term ‘watershed’ is used to describe the region of tendon with poor bloody supply – predisposing to tendon rupture.
Insertion of tendon into calcaneus
This is a less common location for an achilles rupture. In this scenario, the achilles tendon ruptures directly off its insertion into the heel bone (calcaneus). This is typically seen in patients with underlying achilles tendinosis.
Musculoteninous Junction
Achilles ruptures in this area occur closer to the calf muscle bellies. This are best managed non-operatively with functional rehabilitation in combination with a dedicated rehabilitation team.
Minimally Invasive Achilles Rupture Repair
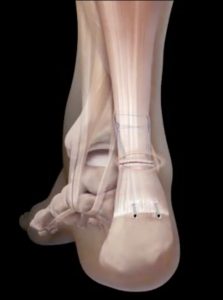
The majority of achilles ruptures occur at the ‘watershed’ zone of the tendon, and are amenable to this technique. The technique itself, involves making a small horizontal incision at the level of the achilles rupture, on the back of the calf.
A specialised ‘jig’ is passed through this small incision, and used to secure the proximal (top) part of the tendon with sutures. These sutures are retrieved through the distal (bottom) part of the achilles tendon, and secured into the heel bone via the use of specialised anchors . This achieves very strong fixation of the sutures, and allows for early mobility.
The procedure is typically performed as a day procedure.

Recovery and Rehabilitation
What to expect following your procedure
The above surgical technique allows for early mobility and weight bearing. Weight bearing is commenced immediately with the addition of a postoperative boot. Depending on any other risk factors that may be present, patients are typically commenced on aspirin to reduce the risk of developing a blood clot. A wound review is performed 2 weeks following surgery, and a structured rehabilitation program is commenced with the support of dedicated sports physiotherapists. Progressive range of motion exercises and a strengthening program is initiated.
Ask the Surgeon
Visit us on Facebook to "Ask the Surgeon"
Want to ask us a question? Visit us on Facebook and post your question. Your questions will be public, and answered as soon as possible.
Contact Us
Tel: (08) 7099 0188
Address: 94-96 Fullarton Rd, Norwood, 5067
Orthopaedics 360
Orthopaedics 360
P: (08) 7099 0188
F: (08) 7099 0171
Southern Specialist Centre
Orthopaedics 360
P: (08) 7099 0188
F: (08) 7099 0171
Health @ Hindmarsh
Orthopaedics 360
P: (08) 7099 0188
F: (08) 7099 0171